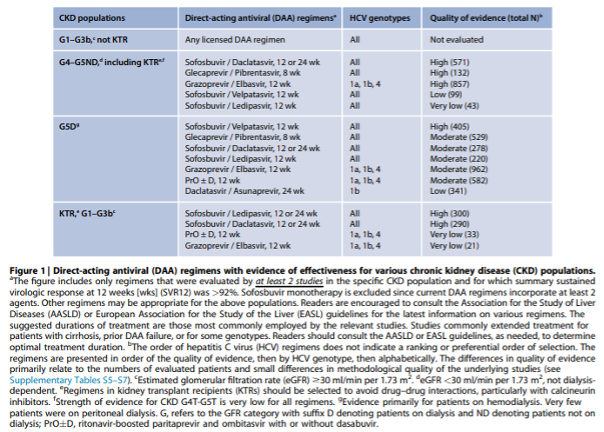
2.1: We recommend that all patients with CKD (G1-G5), on dialysis (G5D), and kidney transplant recipients (G1T-G5T) with HCV be evaluated for direct-acting antiviral (DAA)-based therapy as outlined in Figure 1 (1A).
2.1.1: We recommend that the choice of specific regimen be based on prior treatment history, drug–drug interactions, GFR, stage of hepatic fibrosis, kidney and liver transplant candidacy, and comorbidities (1A). If pangenotypic regimens are not available, HCV genotype (and subtype) should guide the choice of treatment (Figure 1).
2.1.2: Treat kidney transplant candidates in collaboration with the transplant center to optimize timing of therapy (Not Graded).
2.1.3: We recommend pre-treatment assessment for drug–drug interactions between the DAA-based regimen and other concomitant medications including immunosuppressive drugs in kidney transplant recipients (1A).
2.1.4: We recommend that calcineurin inhibitor levels be monitored during and after DAA treatment in kidney transplant recipients (1B).
2.2: All patients with CKD (G1-G5), on dialysis (G5D), and kidney transplant recipients (G1T-G5T) with HCV should undergo testing for hepatitis B virus (HBV) infection prior to DAA therapy (Not Graded).
2.2.1: If hepatitis B surface antigen [HBsAg] is present, the patient should undergo assessment for HBV therapy (Not Graded).
2.2.2: If HBsAg is absent but markers of prior HBV infection (HBcAb-positive with or without HBsAb) are detected, exclude HBV reactivation with HBV DNA testing if levels of liver function tests rise during DAA therapy (Not Graded).
NFN advies:
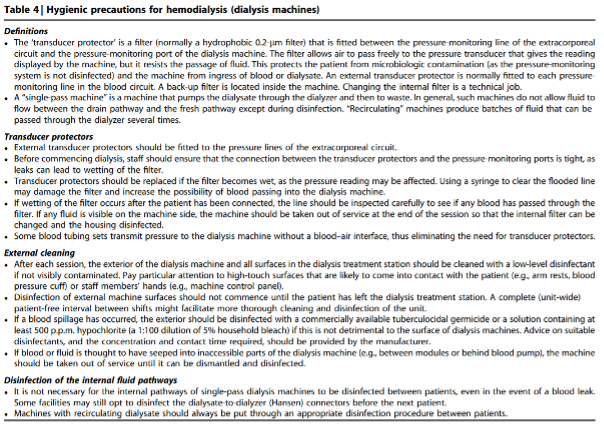
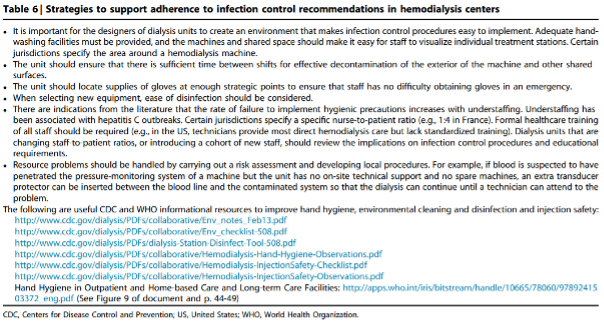
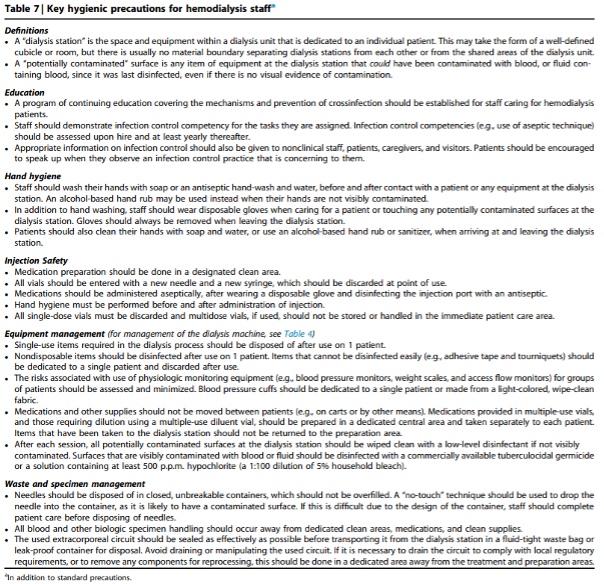
3.1: We recommend that hemodialysis facilities adhere to standard infection control procedures including hygienic precautions that effectively prevent transfer of blood and blood-contaminated fluids between patients to prevent transmission of blood-borne pathogens (see Table 1) (1A).
|
Table 1 | Infection control practices (“hygienic precautions”) particularly relevant for preventing HCV transmission |
|
3.1.1: We recommend regular observational audits of infection control procedures in hemodialysis units (1C).
3.1.2: We recommend not using dedicated dialysis machines for HCV-infected patients (1D).
3.1.3: We suggest not isolating HCV-infected hemodialysis patients (2C).
3.1.4: We suggest that the dialyzers of HCV-infected patients can be reused if there is adherence to standard infection control procedures (2D).
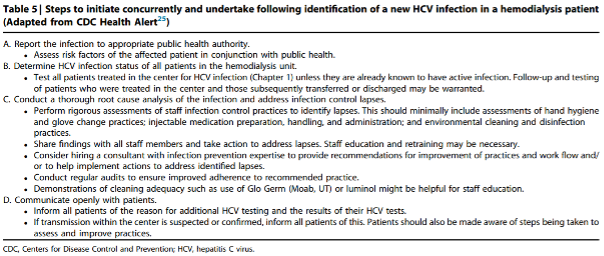
3.2: We recommend that hemodialysis centers examine and track all HCV test results to identify new cases of HCV infections in their patients (1B).
3.2.1: We recommend that aggressive measures be taken to improve hand hygiene (and proper glove use), injection safety, and environmental cleaning and disinfection when a new case of HCV is identified that is likely to be dialysis-related (1A).
3.3: Strategies to prevent HCV transmission within hemodialysis units should prioritize adherence to standard infection control practices and should not primarily rely upon the treatment of HCV-infected patients (Not Graded).
Table 3 | Factors and lapses in infection control practices associated with transmission of HCV infection in dialysis units
Commentaar
Ter preventie van de verspreiding van HCV dienen de juiste methoden en producten te worden toegepast zoals beschreven in de multidisciplinaire richtlijn ‘Hemodialyse’ van Samenwerkingsverband Richtlijnen en Infectiepreventie (SRI), die in najaar 2024 zal verschijnen.
4.1.1: We recommend kidney transplantation as the best therapeutic option for patients with CKD G5 irrespective of presence of HCV infection (1A).
Commentaar
De keuze voor het starten van nierfunctievervangende therapie en welke vorm (dialyse of niertransplantatie, komt tot stand middels gedeelde besluitvorming en dient niet beïnvloed te worden door de aan- of afwezigheid van een HCV infectie [7].
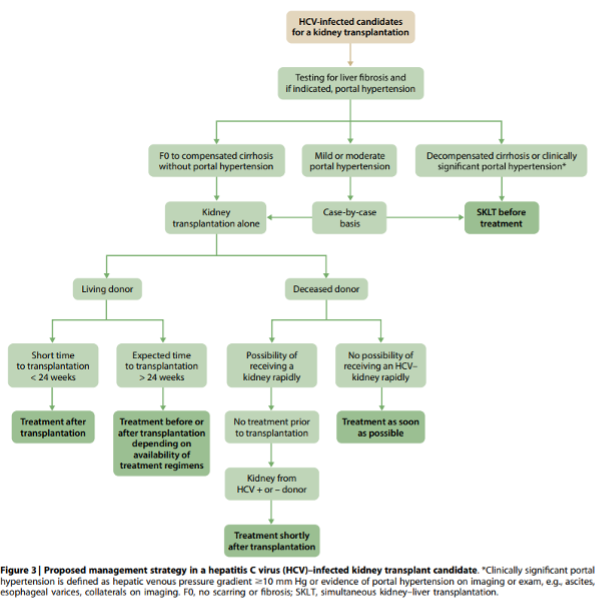
4.1.2: We suggest that all kidney transplant candidates with HCV be evaluated for severity of liver disease and presence of portal hypertension prior to acceptance for kidney transplantation (2D).
4.1.2.1: We recommend that patients with HCV, compensated cirrhosis, and no portal hypertension undergo isolated kidney transplantation and that patients with decompensated cirrhosis or clinically significant portal hypertension (i.e., hepatic venous pressure gradient ≥10 mm Hg or evidence of portal hypertension on imaging or exam) undergo a simultaneous liver–kidney transplantation (1B). Treatment of those with mild-to-moderate portal hypertension should be determined on a case-by-case basis.
4.1.2.2: We recommend referring patients with HCV and decompensated cirrhosis for combined liver–kidney transplantation (1B).
4.1.3: Timing of HCV treatment in relation to kidney transplantation (before vs. after) should be based on donor type (living vs. deceased donor), wait-list times by donor type, center-specific policies governing the use of kidneys from HCV-infected deceased donors, and severity of liver fibrosis (Not Graded).
4.1.3.1: We recommend that all kidney transplant candidates with HCV be considered for DAA therapy, either before or after transplantation (1A).
4.1.3.2: We suggest that HCV-infected kidney transplant candidates with a living kidney donor be considered for treatment before or shortly after transplantation depending on the anticipated timing of transplantation (2B).
Commentaar
Geen aanvullingen voor Nederlandse situatie.
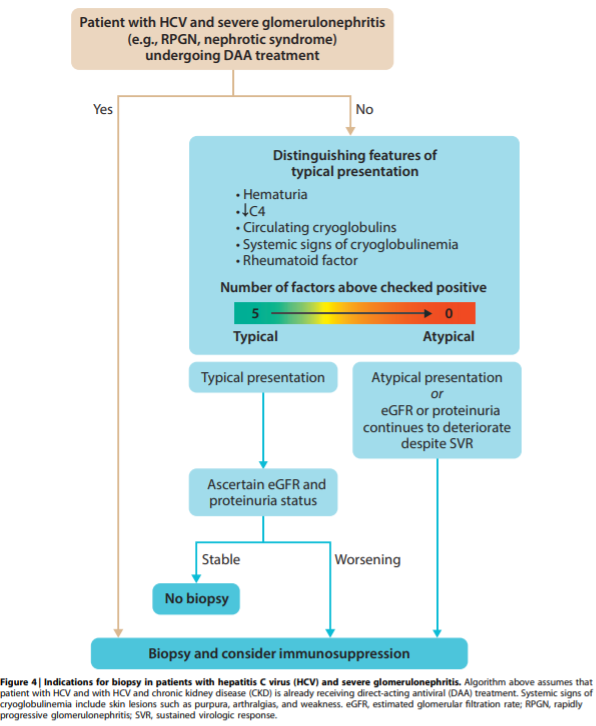
5.1: HCV-infected patients with a typical presentation of immune-complex proliferative glomerulonephritis can be managed without a confirmatory kidney biopsy. However, a biopsy may be indicated in certain clinical circumstances (Figure 4) (Not Graded).
5.2: We recommend that patients with HCV-associated glomerulonephritis receive antiviral therapy (1A).
5.2.1: We recommend that patients with HCV-associated glomerulonephritis, stable kidney function, and without nephrotic syndrome be treated with DAAs prior to other treatments (1C).
5.2.2: We recommend that patients with cryoglobulinemic flare or rapidly progressive glomerulonephritis be treated with both DAAs and immunosuppressive agents with or without plasma exchange (1C).
5.2.2.1: The decision whether to use immunosuppressive agents in patients with nephrotic syndrome should be individualized (Not Graded).
5.2.3: We recommend immunosuppressive therapy in patients with histologically active HCV-associated glomerulonephritis who do not respond to antiviral therapy, particularly those with cryoglobulinemic kidney disease (1B).
5.2.3.1: We recommend rituximab as the first-line immunosuppressive treatment (1C).
Commentaar
Geen aanvullingen voor de Nederlandse situatie.